Many people assume that a polygraph examination begins the moment the sensors are placed on the examinee’s body. In reality, the foundations of a scientifically sound and professionally defensible examination are laid well before the testing phase commences.
At The Centre for Forensic Neuroscience, we regard comprehensive pre-examination screening not as an administrative formality, but as an essential component of responsible forensic psychophysiology.
This article explains why. It examines the physiological systems that underpin polygraph recordings, identifies medical and psychological conditions that may influence those systems, and describes how structured screening protects both the examinee and the integrity of the examination itself.
“Polygraphy presupposes that the subject will have a consistent and measurable physiologic response when he or she attempts to deceive the interviewer.”
— Cook & Mitschow (2019), Federal Practitioner
If that presupposition is not examined carefully before testing begins, the scientific basis of the entire examination is placed at risk.
What Does a Polygraph Actually Measure?
It is important to be clear about what a polygraph instrument does — and what it does not do. A polygraph does not detect lies. Rather, it records physiological changes that occur in response to psychologically significant stimuli, such as carefully formulated test questions. The examiner then analyses the pattern and magnitude of those changes to reach a professional opinion about the examinee’s responses.
The physiological channels typically monitored during a modern polygraph examination include:
- Cardiovascular activity — heart rate, blood pressure, and pulse amplitude
- Respiratory patterns — rate, depth, and regularity of breathing
- Electrodermal activity (EDA) — changes in electrical conductance at the skin surface, reflecting sweat gland activity
As Cook and Mitschow (2019) describe, “a standard polygraph measures respiration, heart rate, BP [blood pressure], and sudomotor function (sweating).” Each of these measures is governed by the autonomic nervous system (ANS) — the division of the nervous system responsible for regulating involuntary bodily functions.
Understanding the ANS is therefore fundamental to understanding both how polygraph examinations work and why pre-examination screening is essential.
The Autonomic Nervous System: A Brief Overview
The autonomic nervous system controls physiological processes that occur largely without conscious awareness. It regulates heart rate, blood pressure, respiration, digestion, pupil dilation, and sweating, among other functions. The ANS comprises two principal branches:
The Sympathetic Nervous System
The sympathetic branch is often characterised as the body’s “fight or flight” system. When activated — whether by physical threat, psychological stress, or emotionally significant stimuli — it produces a cascade of physiological effects:
- Increased heart rate and blood pressure, driven by the release of catecholamines (adrenaline and noradrenaline) acting on β-adrenergic receptors in cardiac muscle and blood vessels (Ladage et al., 2013)
- Increased sweat gland activity, which alters the electrical conductance of the skin — the basis of electrodermal activity measurement
- Changes in respiratory rate and depth, reflecting arousal-related shifts in breathing patterns
- Redistribution of blood flow away from the digestive system and towards skeletal muscles
These responses evolved to prepare the organism for rapid action. In the context of a polygraph examination, sympathetic activation in response to relevant test questions provides one of the key physiological signals recorded and analysed by the examiner.
The Parasympathetic Nervous System
The parasympathetic branch is often described as the “rest and digest” system. It acts to counterbalance sympathetic activation, promoting recovery and maintaining homeostasis. Its effects include:
- Reduced heart rate, mediated by the vagus nerve acting on the sinoatrial node
- Lowered blood pressure
- Slower, deeper breathing patterns
- Promotion of digestive activity
The dynamic interplay between sympathetic and parasympathetic activity — known as autonomic balance — determines the baseline physiological state against which polygraph responses are measured. Heart rate variability (HRV), the beat-to-beat variation in cardiac rhythm, is widely used in clinical and research settings as an index of this balance (Shaffer & Ginsberg, 2017).
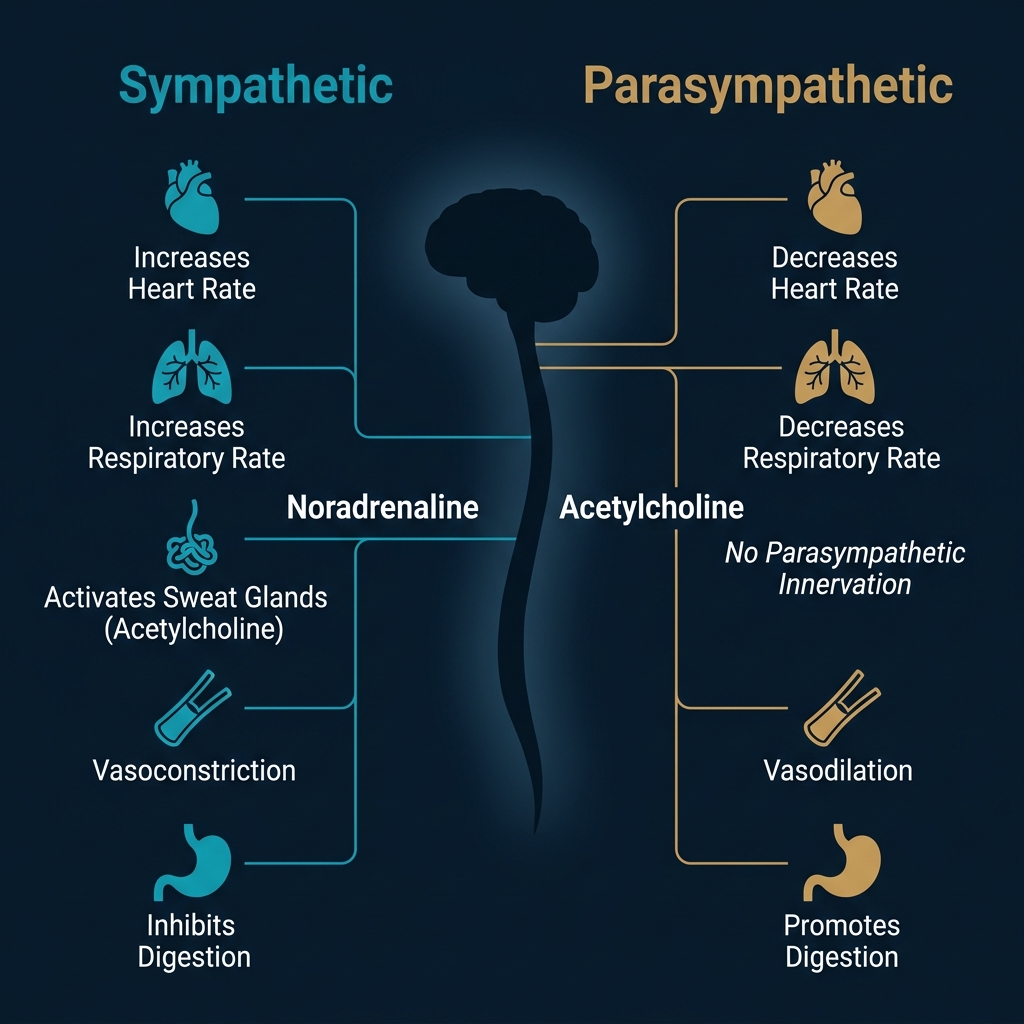
Figure 1. The sympathetic and parasympathetic branches of the autonomic nervous system and their opposing effects on key physiological systems measured during polygraph examination.
Why These Systems Matter for Polygraph Examination
The polygraph works on the principle that psychologically significant stimuli — such as questions that are relevant to the matter under investigation — will produce a measurable shift in autonomic activity relative to comparison or irrelevant questions. As Cook and Mitschow (2019) explain, the examiner “compares the changes in vital signs and skin conduction to the baseline measurements generated during the pretest interview and during control questions.”
This approach relies on several implicit assumptions:
- The examinee’s autonomic nervous system is functioning within broadly normal parameters
- The physiological responses recorded are genuinely stimulus-driven, rather than artefacts of underlying medical conditions or medication effects
- The examinee is capable of producing differential physiological responses to different types of questions
When any of these assumptions is compromised — by disease, medication, substance use, psychological disturbance, or other factors — the examiner’s ability to interpret the physiological data reliably may be diminished. This is precisely why pre-examination screening exists.
The Physiological Channels in Detail
Cardiovascular Responses
During a polygraph examination, cardiovascular activity is monitored through changes in heart rate, blood pressure, and pulse amplitude. These variables are primarily regulated by the sympathetic and parasympathetic branches of the ANS acting on the heart and vasculature. Sympathetic activation increases heart rate and blood pressure through β-adrenergic stimulation, whilst parasympathetic (vagal) input slows heart rate.
The examiner is looking for relative changes — subtle but consistent differences in cardiovascular response between relevant questions and comparison questions. Any condition that disrupts normal cardiovascular regulation, reduces heart rate variability, or introduces arrhythmias may obscure or distort these critical comparisons.
Respiration
Breathing is monitored using pneumograph components, typically strain gauges placed around the chest and abdomen. The examiner assesses respiratory rate, depth, and regularity. Sympathetic arousal typically produces increases in respiratory rate and may alter breathing depth, whilst deliberate breathing manipulation (a common countermeasure attempt) produces characteristic patterns that trained examiners are taught to identify.
Respiratory disorders that alter baseline breathing patterns, or medications that suppress respiratory drive, may complicate the interpretation of breathing-related data.
Electrodermal Activity
Electrodermal activity — sometimes referred to as galvanic skin response or skin conductance — is measured by passing a small, imperceptible electrical current between electrodes attached to the fingertips. Changes in skin conductance reflect the activity of eccrine sweat glands, which are innervated exclusively by the sympathetic branch of the ANS (Boucsein, 2012).
This makes EDA a particularly valuable channel in polygraph examination: it provides a relatively “pure” measure of sympathetic activation, unmodulated by parasympathetic counterbalancing. As Cook and Mitschow (2019) note, “human sweat contains a variety of cations and anions — mostly sodium and chloride, but also potassium, bicarbonate, and lactate. The presence of these electrolytes alter electrical conduction at the skin surface when sweat is released.”
Any condition that impairs sweat gland function — whether through peripheral neuropathy, medication effects, or systemic disease — has the potential to attenuate or abolish the electrodermal responses upon which part of the polygraph analysis depends.
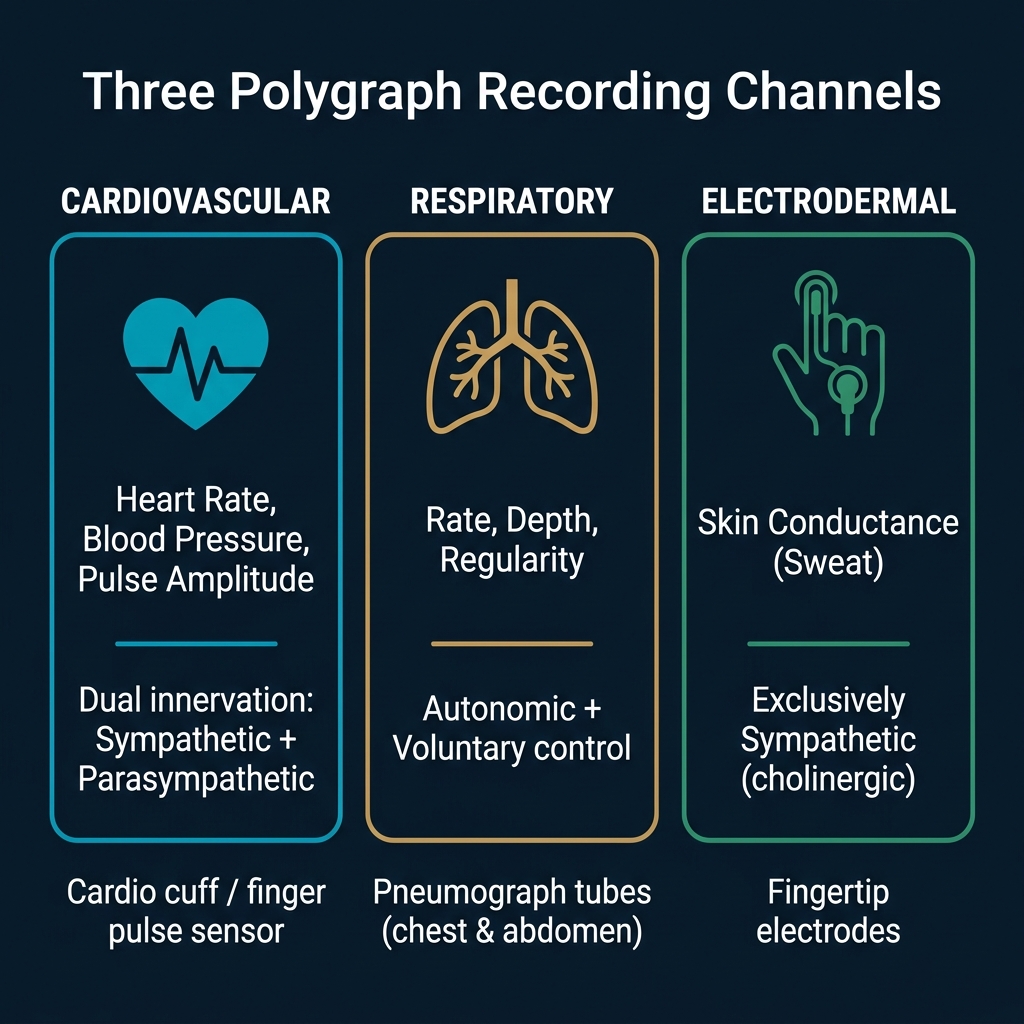
Figure 2. The three primary polygraph channels and their governing autonomic pathways. The electrodermal channel is exclusively sympathetic, making it uniquely sensitive to conditions and medications that affect sympathetic cholinergic function.
How Medical Conditions May Influence Polygraph Recordings
A wide range of medical conditions can affect the autonomic nervous system in ways that may be relevant to polygraph examination. It is important to emphasise that the presence of a medical condition does not automatically prevent an examination from taking place. However, these conditions must be identified and assessed before testing proceeds, so that the examiner can make an informed judgement about examination suitability and, where appropriate, adapt the testing approach.
The following sections draw on the peer-reviewed literature, including the comprehensive review by Cook and Mitschow (2019), to illustrate the scope of conditions that warrant consideration.
Diabetes and Autonomic Neuropathy
Diabetic autonomic neuropathy is one of the most well-documented causes of autonomic dysfunction. Cook and Mitschow (2019) observe that “patients with diabetes mellitus often have an elevated resting heart rate and low heart rate variability due to dysregulated β-adrenergic activity” (Thaung et al., 2015). Autonomic neuropathy in diabetes can affect cardiovascular reflexes, sudomotor (sweating) function, and baroreceptor sensitivity.
The clinical implications for polygraph examination may be significant, depending on the nature and severity of any autonomic involvement. Reduced heart rate variability may diminish the examiner’s ability to detect differential cardiovascular responses, whilst impaired sweat gland innervation may blunt electrodermal activity. As Cook and Mitschow explain, “the impact of reduced baroreceptor response and reduced heart rate variability could impact the polygraph interpreter’s ability to discern responses using heart rate.”
Vinik and Ziegler (2007) reported that cardiovascular autonomic neuropathy affects approximately 20% of people with diabetes and is associated with reduced heart rate variability, exercise intolerance, and orthostatic hypotension — all of which may be relevant to the examination environment.
Cardiovascular Disease, Hypertension, and Arrhythmias
Conditions affecting the heart and vasculature may be directly relevant to polygraph examination because the cardiovascular channel is one of the primary measures analysed. Hypertension may alter baseline blood pressure and reduce the dynamic range of blood pressure responses. Cardiac arrhythmias — such as atrial fibrillation, ectopic beats, or conduction abnormalities — can introduce irregular heart rhythm patterns that may be difficult to distinguish from stimulus-driven cardiovascular changes.
Congestive heart failure is frequently treated with β-blockers, which, as discussed below, have direct effects on the physiological variables measured by the polygraph. Patients with cardiovascular disease may also take vasodilators, ACE inhibitors, or calcium channel blockers, each of which can influence cardiovascular regulation in ways that may affect polygraph recordings.
Respiratory Disease: Asthma and COPD
Asthma and chronic obstructive pulmonary disease (COPD) may alter respiratory patterns at baseline and in response to stress. Bronchospasm, air trapping, and the use of bronchodilator medications (many of which have sympathomimetic properties) can all influence the respiratory channel recorded during a polygraph examination.
Furthermore, respiratory disease may increase baseline anxiety about the testing environment — particularly if the examinee is concerned about breathing restrictions imposed by the pneumograph components. This heightened baseline anxiety may itself confound the physiological recordings.
Autonomic dysfunction has been documented in COPD, with studies reporting reduced heart rate variability and impaired parasympathetic modulation (Van Gestel & Steier, 2010), both of which are relevant to polygraph interpretation.
Neurological Disorders
Several neurological conditions are associated with autonomic nervous system changes that may be relevant to polygraph examination. The degree of autonomic involvement varies considerably between individuals, between conditions, and over time — reinforcing the importance of individual assessment rather than blanket exclusion.
Parkinson’s Disease
Parkinson’s disease is a neurodegenerative condition characterised not only by motor symptoms but also by significant autonomic dysfunction. Cook and Mitschow (2019) note that “synucleinopathies, such as Parkinson disease, alter cardiovascular reflexes” (Postuma et al., 2013). Patients may experience orthostatic hypotension, reduced heart rate variability, and impaired sudomotor function — potentially affecting all three primary polygraph channels.
Multiple Sclerosis
Multiple sclerosis (MS) involves demyelination and neurodegeneration within the central nervous system, which can disrupt autonomic pathways. Studies have reported cardiovascular autonomic dysfunction, bladder dysfunction, and thermoregulatory impairment in patients with MS (Racosta et al., 2015). The degree of autonomic involvement can vary considerably between individuals and may fluctuate over time, making individual assessment essential.
Epilepsy
Epilepsy is primarily a disorder of cortical excitability, but it is increasingly recognised that seizure disorders can be associated with autonomic disturbances. Ictal and interictal autonomic changes — including alterations in heart rate, blood pressure, and electrodermal activity — have been documented in the literature (Devinsky, 2004). Additionally, many anti-epileptic medications have central nervous system effects that may influence arousal and autonomic reactivity.
Traumatic Brain Injury
Traumatic brain injury (TBI) can produce lasting effects on autonomic regulation, particularly when brainstem structures or the hypothalamus are involved. Autonomic dysfunction following moderate-to-severe TBI may include dysregulation of heart rate, blood pressure, respiratory patterns, and thermoregulation (Baguley et al., 2008). Even mild TBI has been associated with reduced heart rate variability in some studies, suggesting subtle but measurable changes in autonomic function (Hilz et al., 2011).
Mental Health Conditions
Mental health conditions are common in the general population and are frequently encountered in polygraph practice. The presence of a mental health diagnosis does not preclude examination, but may influence the autonomic baseline and the pattern of physiological responses observed during testing. The following conditions warrant particular consideration.
Anxiety Disorders and Panic Disorder
Anxiety disorders are characterised by heightened sympathetic activation and may produce elevated baseline levels of cardiovascular and electrodermal activity. Panic disorder, in particular, involves episodes of acute sympathetic arousal that may occur unpredictably. During a polygraph examination, elevated baseline arousal in an anxious examinee may reduce the differential between responses to relevant and comparison questions, potentially obscuring meaningful physiological signals.
Generalised anxiety disorder has been associated with reduced heart rate variability and elevated resting heart rate (Chalmers et al., 2014), findings that are directly relevant to the cardiovascular channel in polygraph testing.
Post-Traumatic Stress Disorder (PTSD)
PTSD is characterised by a constellation of symptoms including hyperarousal, re-experiencing, avoidance, and emotional numbing. The hyperarousal symptoms — including exaggerated startle response, hypervigilance, and physiological reactivity to trauma-related cues — reflect persistent sympathetic nervous system dysregulation (Pole, 2007).
In a polygraph context, PTSD presents particular challenges. If the subject matter of the examination is related to the individual’s traumatic experiences, the physiological responses recorded may reflect trauma-related reactivity rather than deception-related arousal. Additionally, the examination environment itself — including the authority dynamics, the interrogative structure, and physical confinement — may trigger trauma responses in some individuals.
Depression
Major depressive disorder has been associated with autonomic dysregulation, including reduced heart rate variability, elevated resting heart rate, and blunted cardiovascular reactivity to psychological stressors (Kemp et al., 2010). Electrodermal hyporesponsiveness — reduced skin conductance responses — has also been reported in depression (Dawson et al., 2007).
These patterns may attenuate the physiological responses that the polygraph examiner relies upon for analysis, potentially increasing the risk of inconclusive or difficult-to-interpret results.
Chronic Pain
Chronic pain conditions are associated with significant autonomic nervous system changes, including altered sympathovagal balance, reduced heart rate variability, and changes in electrodermal activity (Tracy et al., 2016). Pain itself produces sympathetic activation that may elevate baseline physiological levels and reduce the dynamic range available for stimulus-driven responses.
Furthermore, chronic pain is frequently treated with opioid analgesics, gabapentinoids, and other medications that have effects on central nervous system arousal and autonomic function.
Sleep Disorders
Sleep disorders — particularly obstructive sleep apnoea (OSA) — are associated with significant autonomic dysfunction. OSA produces repeated episodes of hypoxia and sympathetic activation during sleep, leading to sustained changes in cardiovascular autonomic regulation, including elevated daytime blood pressure, reduced heart rate variability, and increased sympathetic tone (Somers et al., 2008).
Insufficient sleep, regardless of the underlying cause, impairs cognitive function, reduces attention, and may alter physiological reactivity in ways that affect the reliability of polygraph examination.
Endocrine Disorders
Endocrine conditions, particularly thyroid dysfunction and adrenal disorders, can influence autonomic function. Hyperthyroidism can produce a state of sympathetic overactivity, with elevated heart rate, increased blood pressure, tremor, and excessive sweating. Hypothyroidism, conversely, may produce bradycardia, reduced cardiovascular reactivity, and diminished electrodermal activity.
Cushing’s syndrome and adrenal insufficiency (Addison’s disease) alter cortisol regulation, which in turn affects cardiovascular function and autonomic reactivity. Phaeochromocytoma — a rare catecholamine-secreting tumour — can produce dramatic and unpredictable surges in blood pressure and heart rate.
“A variety of diseases from alcohol use disorder to rheumatoid arthritis can affect the ANS. In addition, a multitude of commonly prescribed drugs can affect the ANS.”
— Cook & Mitschow (2019)
Medications That May Influence Polygraph Recordings
Medications represent another significant category of factors that must be assessed before a polygraph examination. Cook and Mitschow (2019) emphasise that “of the 10 most prescribed medications of 2016, 5 have direct effects on the ANS or the variables measured by the polygraph machine.” The implications for pre-examination screening are clear.
Beta-Blockers
Beta-adrenergic blocking agents are among the most commonly prescribed medications in the United Kingdom. As Cook and Mitschow (2019) explain, “β blockers reduce β adrenergic receptor activation in cardiac muscle and blood vessels, reducing heart rate, heart rate variability, cardiac contractility, and BP.” They are prescribed for conditions including hypertension, heart failure, angina, arrhythmias, migraine prophylaxis, essential tremor, and — importantly — anxiety-related conditions such as panic disorder and PTSD.
The consequence for polygraph examination is direct: “a patient taking β blockers will have a blunted physiologic response to stress and have an increased likelihood of an inconclusive or false-negative polygraph exam” (Cook & Mitschow, 2019).
Antidepressant Medications
Antidepressants exert a range of effects on autonomic function depending on their pharmacological class:
- Tricyclic antidepressants (TCAs) have significant anticholinergic properties that reduce heart rate variability, produce dry mouth, and may diminish sweating — directly affecting multiple polygraph channels
- Selective serotonin reuptake inhibitors (SSRIs) have been shown to reduce heart rate variability and may affect electrodermal responses (Licht et al., 2008)
- Serotonin-noradrenaline reuptake inhibitors (SNRIs) may increase heart rate and blood pressure through noradrenergic mechanisms
Anxiolytic Medications
Benzodiazepines (such as diazepam, lorazepam, and alprazolam) reduce anxiety by enhancing GABAergic inhibition in the central nervous system. This produces a generalised dampening of physiological arousal, including reduced heart rate, blood pressure, and electrodermal activity. In a polygraph context, anxiolytic medication may attenuate the differential responses upon which analysis depends.
Stimulant Medications
Stimulant medications prescribed for attention deficit hyperactivity disorder (ADHD) — including methylphenidate and amphetamine-based preparations — increase sympathetic nervous system activity. They may elevate baseline heart rate, blood pressure, and electrodermal activity, potentially altering the physiological landscape in ways that affect polygraph interpretation.
Other Medications of Note
Cook and Mitschow (2019) also highlight the effects of over-the-counter medications, noting that “sympathomimetics such as pseudoephedrine or antihistamines with anticholinergic activity like diphenhydramine can both increase heart rate and BP.” Anticholinergic medications, opioid analgesics, antipsychotics, corticosteroids, and medications affecting thermoregulation may all warrant consideration during pre-examination screening.
Alcohol, Recreational Drugs, and Substance Use
Cook and Mitschow (2019) note that “ANS dysfunction is also a common sequela of alcoholism” (Di Ciaula et al., 2016). Both acute intoxication and chronic substance use can alter autonomic function in ways that are relevant to polygraph examination. Acute alcohol intoxication impairs cognitive function and alters cardiovascular and electrodermal responses. Chronic alcohol use is associated with autonomic neuropathy.
Recreational drugs — including cannabis, cocaine, MDMA, and amphetamines — have significant acute effects on autonomic function. Pre-examination screening must therefore include questions about recent alcohol and drug use to determine whether the examinee is in a suitable physiological state for testing.
The Centre’s Structured Pre-Examination Screening Process
At The Centre for Forensic Neuroscience, every polygraph examination is preceded by a structured screening process designed to identify factors that may affect the suitability, validity, or safety of the examination. This process is not optional, and it is not an afterthought — it is an integral part of the examination protocol.
What the Screening Covers
The pre-examination screening assesses a range of factors, including:
- Medical history — cardiovascular, respiratory, neurological, endocrine, and other conditions that may affect autonomic function
- Mental health — current and historical diagnoses, including anxiety disorders, depression, PTSD, and psychotic disorders
- Medication — all current prescribed and over-the-counter medications, with particular attention to those known to affect the autonomic nervous system
- Neurological disorders — conditions affecting the central or peripheral nervous system, including epilepsy, traumatic brain injury, multiple sclerosis, and Parkinson’s disease
- Alcohol and drug use — recent and habitual use of alcohol and recreational substances
- Language comprehension — the examinee’s ability to understand the language in which the examination will be conducted, and whether an interpreter is required
- Cognitive ability — whether the examinee has sufficient cognitive capacity to understand the questions, the testing process, and the concept of informed consent
- Safeguarding concerns — vulnerability factors, including age, learning disability, mental health crisis, and risk of self-harm
- Coercion — whether the examinee is attending voluntarily and free from improper pressure, intimidation, or duress
- Examination suitability — an overall professional judgement about whether the examination can be conducted ethically and is likely to produce reliable results
- Legal and ethical considerations — including the intended use of the results, confidentiality arrangements, and whether there are any conflicts of interest
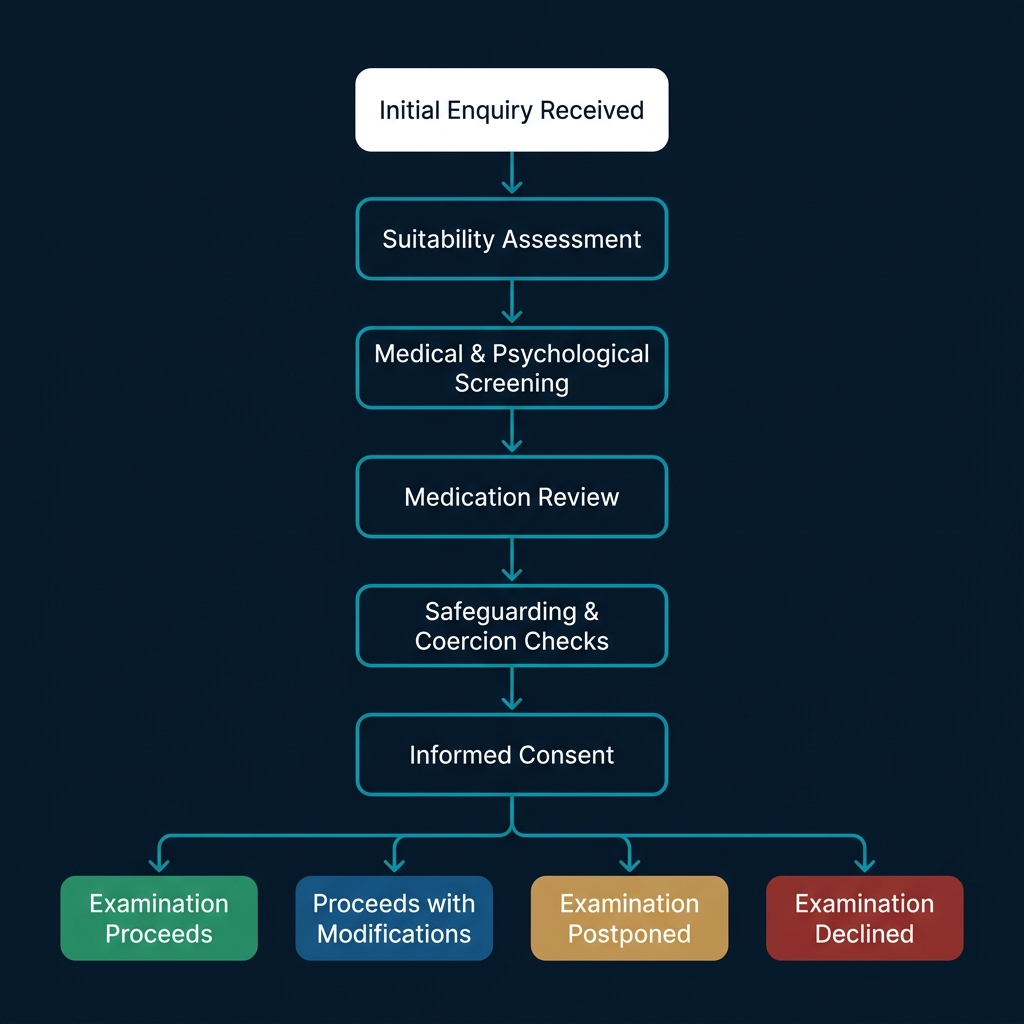
Figure 3. The structured pre-examination screening pathway used by The Centre for Forensic Neuroscience, showing the four possible outcomes: examination proceeds, proceeds with modifications, postponed, or declined.
Important: What the Screening Is — and What It Is Not
The pre-examination screening process is not a medical assessment. It does not diagnose disease, confirm or exclude medical conditions, or replace the advice of a qualified medical practitioner. It is a structured suitability assessment, designed solely to determine whether a polygraph examination can be conducted safely, ethically, and in a manner likely to produce scientifically interpretable results.
Where an examinee discloses a medical condition or medication, this information is considered only insofar as it may influence autonomic nervous system function during the examination. In some cases, the examiner may recommend that the examinee seeks advice from their general practitioner or treating clinician before the examination proceeds.
The screening process does not guarantee that an examination will produce conclusive or accurate results. It is a risk-mitigation measure — one component of a professionally structured examination protocol.
Why We Ask About Your Medical History
As part of the pre-examination screening process, we ask examinees to provide information about their medical history, current medications, and psychological health. We recognise that this information is personal and sensitive.
Health information disclosed during screening is treated as confidential. Only information that is directly relevant to the assessment of examination suitability is collected. This information is:
- Used solely to assess whether the examination can be conducted safely and to a scientifically defensible standard
- Not shared with third parties unless required by law or with the examinee’s explicit consent
- Stored securely in accordance with the Centre’s data protection policies
- Processed in accordance with the UK General Data Protection Regulation (UK GDPR) and the Data Protection Act 2018, under the lawful basis of legitimate interest and, where applicable, explicit consent for special category data
Further details are set out in our Privacy Policy.
Who the Screening Protects
Examinee welfare. The primary obligation of any professional examiner is to ensure that the examination does not cause harm. Screening identifies medical, psychological, or situational factors that might make testing inappropriate or distressing.
Scientific validity. If the examiner is unaware of factors affecting the examinee’s autonomic function, the physiological recordings cannot be interpreted with confidence. As Cook and Mitschow (2019) state, “individuals with ANS dysfunction that causes blunted physiologic responses could have inconclusive or potentially worse false-negative polygraph results due to lack of variation between control and target questions.”
Interpretation of physiological recordings. Even when an examination proceeds, knowledge of an examinee’s medical conditions and medications allows the examiner to contextualise the physiological data appropriately and avoid misattributing responses.
Legal defensibility. In legal and professional contexts, a polygraph examination may be subject to scrutiny. An examination conducted without adequate screening is vulnerable to challenge on the grounds that relevant factors were not considered.
Professional ethics. Accepted principles of professional forensic practice and the standards maintained by the American Polygraph Association require that examiners exercise due diligence in assessing examination suitability. Screening fulfils this ethical obligation.
Possible Outcomes of Screening
Following pre-examination screening, several outcomes are possible:
- The examination proceeds as planned. No factors have been identified that would compromise the validity or safety of the examination.
- The examination proceeds with modifications. For example, additional rest breaks may be incorporated, the testing environment may be adjusted, or the examiner may give particular weight to certain physiological channels during analysis.
- The examination is postponed. Temporary factors — such as acute illness, recent medication changes, sleep deprivation, or emotional distress — may resolve with time, making a future examination appropriate.
- The examination is declined. Where factors are present that would fundamentally compromise the validity of the examination or risk harm to the examinee, the responsible course of action is not to proceed.
“Dysautonomias may be an underappreciated cause of error in polygraph interpretation. Polygraph examiners and DoD agencies should be aware of the potential for these disorders to interfere with interpretation of results.”
— Cook & Mitschow (2019)
Why Screening Distinguishes Professional Practice
It is not uncommon for people to assume that a polygraph examination is a straightforward procedure that begins when the sensors are attached and concludes when a result is given. This assumption overlooks the considerable scientific and clinical groundwork that must precede any responsible examination.
Professional forensic practice begins with a different question entirely: should this examination take place at all?
Determining the answer to that question requires a structured assessment of the examinee’s physical health, mental health, medication, cognitive capacity, language comprehension, vulnerability, and the circumstances under which they are attending. It requires knowledge of how the autonomic nervous system functions, what can disrupt it, and how those disruptions affect the physiological data upon which the examination depends.
At The Centre for Forensic Neuroscience, comprehensive pre-examination screening is one of the defining features of our practice. We do not regard it as an inconvenience or a barrier to testing. We regard it as the scientific and ethical foundation upon which every credible examination is built.
As Cook and Mitschow (2019) concluded in their review, “the polygraph examiner and the physician must be aware of the effect of autonomic dysfunction and of the medications that affect the ANS.” We agree — and we believe this awareness must be systematically applied, not left to chance.
Healthy Ageing, Individual Variation, and Why Blanket Exclusion Is Not the Answer
It is important to recognise that autonomic nervous system function is not uniform across the population. Even in the absence of diagnosed disease, autonomic responsiveness varies between individuals as a result of age, fitness, genetics, habitual medication use, and a range of other factors.
Age-related changes in autonomic function are well documented. Heart rate variability tends to decline with advancing age, baroreceptor sensitivity may be reduced, and electrodermal responsiveness can diminish (Moodithaya & Avadhany, 2012). These changes do not constitute disease, but they may influence the physiological data recorded during a polygraph examination and should be considered during analysis.
Equally, many individuals with diagnosed medical conditions — including well-controlled diabetes, stable hypertension, or treated depression — retain sufficient autonomic responsiveness for a meaningful examination to be conducted. The purpose of screening is not to exclude, but to assess. A suitability-led approach ensures that each case is evaluated on its own merits, taking account of the specific condition, its severity, the current treatment regimen, and the individual’s presentation on the day of the examination.
Blanket exclusion policies — refusing to test anyone with a particular diagnosis — are neither scientifically justified nor professionally defensible. They risk denying examinations to individuals who are fully suitable, whilst offering false reassurance in cases where undisclosed or unrecognised conditions are present. Individual assessment is the only responsible approach.
Key Takeaways
- The polygraph does not detect lies. It records physiological changes — governed by the autonomic nervous system — associated with psychologically significant stimuli.
- The autonomic nervous system can be affected by a wide range of conditions, including diabetes, cardiovascular disease, respiratory disease, neurological disorders, mental health conditions, chronic pain, sleep disorders, and endocrine dysfunction.
- Many commonly prescribed medications influence autonomic function, including beta-blockers, antidepressants, anxiolytics, stimulants, and anticholinergic agents.
- Unrecognised autonomic dysfunction may lead to unreliable results, including increased risk of inconclusive outcomes or false-negative findings.
- Pre-examination screening is not an administrative exercise — it is a scientifically necessary process that protects the examinee, the validity of the examination, and the professional standing of the examiner.
- The presence of a medical condition or medication does not automatically prevent examination. However, it must be assessed by the examiner before a decision about suitability is made.
- A scientifically defensible polygraph examination begins long before the sensors are attached.
Conclusion
The peer-reviewed literature is clear: the physiological systems measured during a polygraph examination are subject to a wide range of medical, pharmacological, psychological, and situational influences. Any of these factors, if unidentified, has the potential to compromise the interpretability of the physiological recordings and, by extension, the validity of the examination itself.
At The Centre for Forensic Neuroscience, we take the position that responsible forensic psychophysiology demands a rigorous, structured approach to pre-examination screening. This is not a commercial differentiator — it is a scientific and ethical imperative. We are prepared to postpone or decline examinations where the evidence suggests that proceeding would not serve the interests of scientific validity, examinee welfare, or professional integrity.
The hallmark of professional polygraph practice is not the willingness to test, but the willingness to recognise when an examination should not proceed.
For solicitors, healthcare professionals, corporate investigators, and members of the public considering a polygraph examination, we would offer this observation: the quality of a polygraph examination cannot be judged solely by the technology used or the result produced. It must also be judged by the care taken — before any sensor is attached — to determine whether the examination should take place at all.
References
Baguley, I. J., Heriseanu, R. E., Cameron, I. D., Nott, M. T., & Slewa-Younan, S. (2008). A critical review of the pathophysiology of dysautonomia following traumatic brain injury. Neurocritical Care, 8(2), 293–300.
Boucsein, W. (2012). Electrodermal activity (2nd ed.). Springer.
Chalmers, J. A., Quintana, D. S., Abbott, M. J.-A., & Kemp, A. H. (2014). Anxiety disorders are associated with reduced heart rate variability: A meta-analysis. Frontiers in Psychiatry, 5, 80.
Cook, G., & Mitschow, C. (2019). Beyond the polygraph: Deception detection and the autonomic nervous system. Federal Practitioner, 36(7), 316–321.
Dawson, M. E., Schell, A. M., & Filion, D. L. (2007). The electrodermal system. In J. T. Cacioppo, L. G. Tassinary, & G. G. Berntson (Eds.), Handbook of psychophysiology (3rd ed., pp. 159–181). Cambridge University Press.
Devinsky, O. (2004). Effects of seizures on autonomic and cardiovascular function. Epilepsy Currents, 4(2), 43–46.
Di Ciaula, A., Grattagliano, I., & Portincasa, P. (2016). Chronic alcoholics retain dyspeptic symptoms, pan-enteric dysmotility, and autonomic neuropathy before and after abstinence. Journal of Digestive Diseases, 17(11), 735–746.
Hilz, M. J., DeFina, P. A., Anders, S., Koehn, J., Lang, C. J., Pauli, E., Flanagan, S. R., & Schwab, S. (2011). Frequency analysis unveils cardiac autonomic dysfunction after mild traumatic brain injury. Journal of Neurotrauma, 28(9), 1727–1738.
Kemp, A. H., Quintana, D. S., Gray, M. A., Felmingham, K. L., Brown, K., & Gatt, J. M. (2010). Impact of depression and antidepressant treatment on heart rate variability: A review and meta-analysis. Biological Psychiatry, 67(11), 1067–1074.
Ladage, D., Schwinger, R. H., & Brixius, K. (2013). Cardio-selective beta-blocker: Pharmacological evidence and their influence on exercise capacity. Cardiovascular Therapeutics, 31(2), 76–83.
Licht, C. M. M., de Geus, E. J. C., Zitman, F. G., Hoogendijk, W. J. G., van Dyck, R., & Penninx, B. W. J. H. (2008). Association between major depressive disorder and heart rate variability in the Netherlands Study of Depression and Anxiety (NESDA). Archives of General Psychiatry, 65(12), 1358–1367.
Pole, N. (2007). The psychophysiology of posttraumatic stress disorder: A meta-analysis. Psychological Bulletin, 133(5), 725–746.
Postuma, R. B., Gagnon, J. F., Pelletier, A., & Montplaisir, J. (2013). Prodromal autonomic symptoms and signs in Parkinson’s disease and dementia with Lewy bodies. Movement Disorders, 28(5), 597–604.
Racosta, J. M., Kimpinski, K., Engstrom, J. W., & Bhatt, D. K. (2015). Autonomic dysfunction in multiple sclerosis. Autonomic Neuroscience: Basic and Clinical, 193, 1–6.
Shaffer, F., & Ginsberg, J. P. (2017). An overview of heart rate variability metrics and norms. Frontiers in Public Health, 5, 258.
Somers, V. K., White, D. P., Amin, R., Abraham, W. T., Costa, F., Culebras, A., Daniels, S., Floras, J. S., Hunt, C. E., Olson, L. J., Pickering, T. G., Russell, R., Woo, M., & Young, T. (2008). Sleep apnea and cardiovascular disease. Journal of the American College of Cardiology, 52(8), 686–717.
Thaung, H. A., Baldi, J. C., Wang, H., et al. (2015). Increased efferent cardiac sympathetic nerve activity and defective intrinsic heart rate regulation in type 2 diabetes. Diabetes, 64(8), 2944–2956.
Tracy, L. M., Ioannou, L., Baker, K. S., Gibson, S. J., Georgiou-Karistianis, N., & Giummarra, M. J. (2016). Meta-analytic evidence for decreased heart rate variability in chronic pain implicating parasympathetic nervous system dysregulation. Pain, 157(1), 7–29.
Moodithaya, S., & Avadhany, S. T. (2012). Gender differences in age-related changes in cardiac autonomic nervous function. Journal of Aging Research, 2012, 679345.
Van Gestel, A. J. R., & Steier, J. (2010). Autonomic dysfunction in patients with chronic obstructive pulmonary disease (COPD). Journal of Thoracic Disease, 2(4), 215–222.
Vinik, A. I., & Ziegler, D. (2007). Diabetic cardiovascular autonomic neuropathy. Circulation, 115(3), 387–397.